Did we need a new shingles vaccine? To answer that question, it helps to have a bit of background on this infection.
Shingles, which is also called herpes zoster, occurs when the chickenpox virus (varicella zoster), which is dormant in those who’ve had the illness, reawakens later in life. Almost all adults older than 40 carry the chickenpox virus—and the older we get, the more the risk of getting shingles climbs. According to the CDC, the infection strikes about 1 million people in the U.S. each year and nearly one in three adults will experience a bout of shingles in their lifetime.
The two to four weeks of shingles, marked by symptoms such as a blistery and painful rash on one side of the body, can be difficult enough. But about one in five people with shingles go on to develop postherpetic neuralgia, or PHN, which is nerve pain that can linger for months or even years.
Since 2006, we’ve had Zostavax—approved for those between 50 and 59 but recommended by the CDC for adults 60 and older—as the sole bulwark against shingles. Zostavax offers 70 percent protection against shingles for people between 50 and 59 but only 18 percent in people 80 and older, according to the Pink Sheet, which reports on the pharmaceutical industry.
When all ages are taken into consideration, Zostavax cuts the chance of shingles by only 51 percent and the risk of PHN by 67 percent.
In addition, Zostavax’s effectiveness appears to last just five years, according to the CDC. And research presented in the fall at IDWeek, an annual meeting for infectious disease professionals, suggests that Zostavax may actually wane after only three years.
The Shingrix vaccine (whose two doses are to be given two to six months apart), according to the CDC, offers 97 percent protection in people in their 50s and 60s and roughly 91 percent protection in those in their 70s and 80s. And it appeared to retain similarly high effectiveness throughout a four-year study period and cut PHN risk by 86 percent.
There are key differences between the ways Shingrix and Zostavax are designed. The new shingles vaccine contains an adjuvant, a substance that boosts the immune system’s response. This may be what makes Shingrix both more effective and longer-lasting, says Schaffner at Vanderbilt.
As with Zostavax, the recommendation is that those who are or will soon be on low-dose immunosuppressive therapy (such as less than 20 mg a day of the steroid prednisone), and those who have recovered from an illness that suppresses the immune system, such as leukemia, can get the vaccine.
Right now, Shingrix is not recommended for older adults who are immunocompromised or are taking moderate to high doses of drugs that suppress the immune system.
But because the new shingles vaccine contains a nonliving viral particle, it may ultimately be deemed appropriate for those with compromised immunity. (Zostavax contains live—although weakened—herpes zoster virus, so those with significantly weakened immune systems should not receive it.) The ACIP will review data on Shingrix in these groups as it becomes available.
“Shingles is a big problem with immunocompromised people,” Schaffner says.
Those who are severely allergic to any component of Shingrix should not get the vaccine, and anyone with active shingles should wait until symptoms resolve. The vaccine hasn’t been studied in pregnant or breastfeeding women.







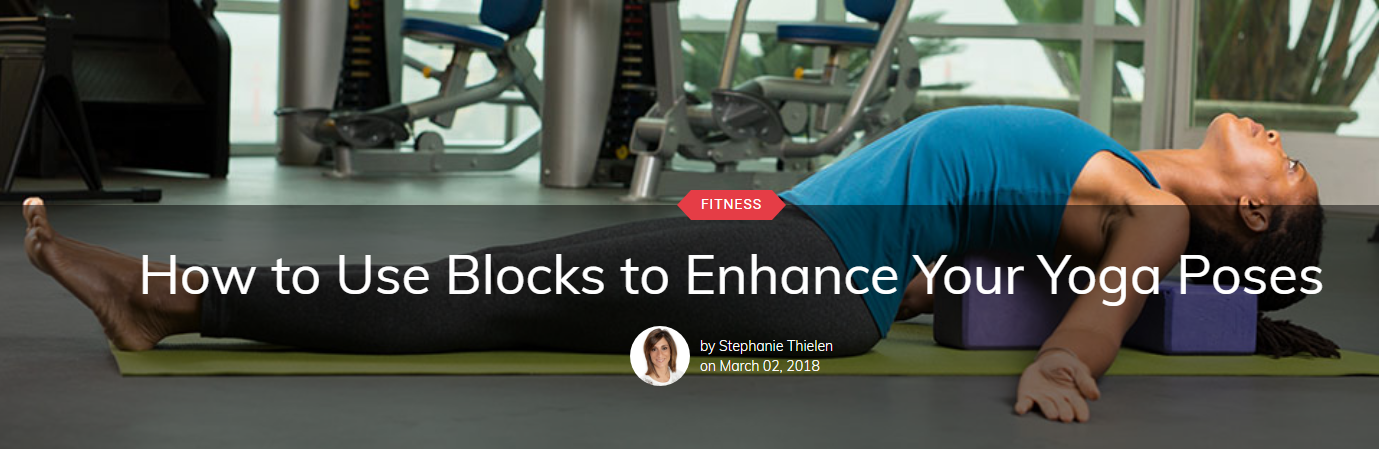 While yoga can help improve flexibility, posture and balance, the practice of yoga offers so much more, including self-reflection, the practice of kindness to ourselves and others, and continued growth and self-awareness. Of course, all of this is much easier to move toward if you can find a sense of comfort in the poses.
While yoga can help improve flexibility, posture and balance, the practice of yoga offers so much more, including self-reflection, the practice of kindness to ourselves and others, and continued growth and self-awareness. Of course, all of this is much easier to move toward if you can find a sense of comfort in the poses.