
Background:
Cardiovascular Disease
Cardiovascular disease is the leading cause of death in America for both men and women and there have been increased incidences over the past few years. 1 Cardiovascular disease can be defined as cardiac arrest, heart attack, arrhythmia, peripheral artery disease, stroke, congestive heart failure, congenital heart disease and many more. 2 Millions of people suffer from a significant risk factor that predisposes them to develop cardiovascular diseases with many going untreated leading to further complications. These risk factors include but are not limited to: Type 2 diabetes, obesity, poor diet and exercise, excessive alcohol use, smoking, hypertension, and dyslipidemia. 1 Inadequate control of these risk factors is what leads to increased rates of death and as of the past year, about half of all Americans experience a cardiac death outside of the hospital. 1 The prevalence and severity of this is of the utmost importance, and new efforts are being made each day in order to reduce those risk factors and prevent more cardiovascular events from happening. The chart below shows the incidence as of 2017 between Indiana and the overall U.S. population.
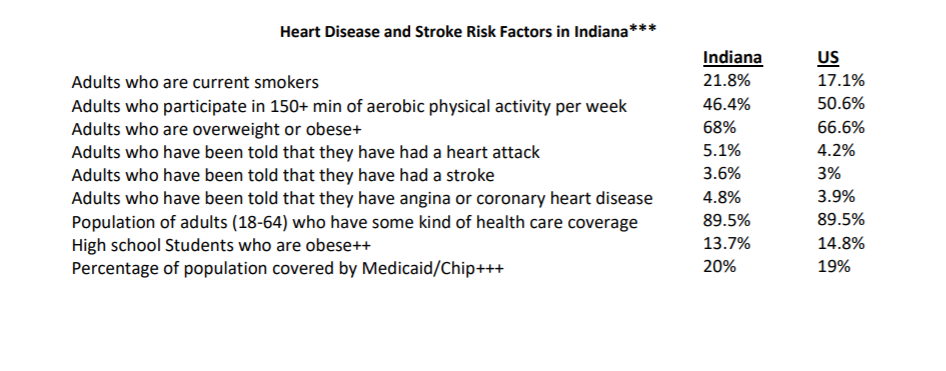
3 Indiana State Fact Sheet. American Heart Association website. https://www.heart.org/-/media/files/about-us/policy-research/fact-sheets/quality-systems-of-care/quality-systems-of-care-indiana.pdf?la=en&hash=96D09D01F6D4695F675C6807B795D1B678A3814A. Accessed November 15, 2019
Homelessness
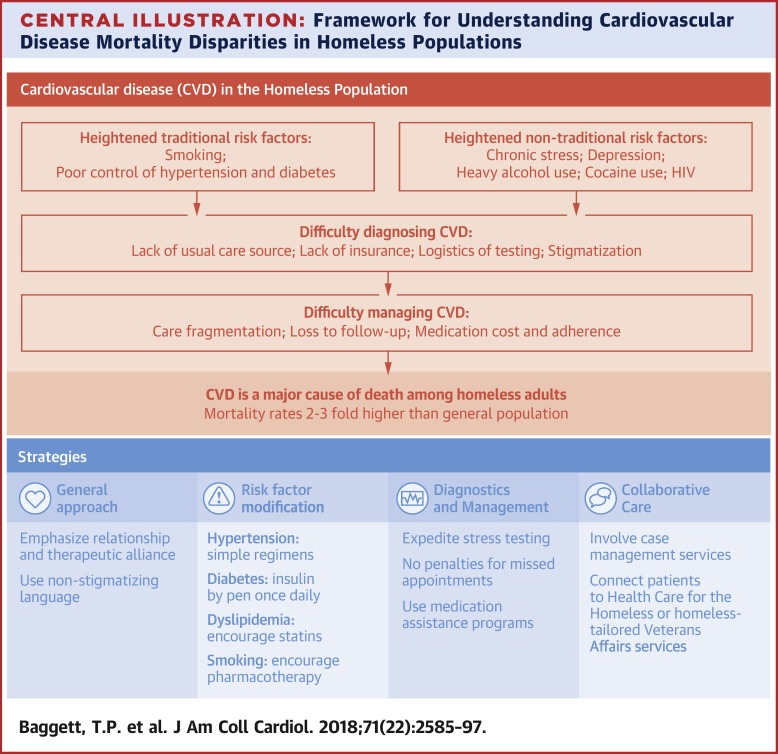
A significant population group that is at an increased risk for cardiovascular events are the homeless communities. About 500,000 are homeless on any given night and about 3.5 million individuals can experience homelessness over the course of the year. 4 In Indiana as of January 2018 about 5,300 people were experiencing homelessness on any given day. 5 While these statistics may fluctuate on a day to day basis, the numbers are alarmingly high that should gravitate our attention. These individuals are included in the heart disease statistics above and the prevalence of the disease states (hypertension, type 2 diabetes, and dyslipidemia) in homeless populations is almost equal to those in non-homeless areas. The problem that we see in homeless areas is that these individuals often go untreated which increases the risk of a cardiovascular event occurring. 4 Not treating these disease states accelerates the incidence of cardiovascular events in these populations leading to a higher mortality rate simply due to inadequate management.. Furthermore, most of the people in the homeless community may not even know they have a disease or that they are living an unhealthy lifestyle which increases the importance of this issue.4 With homeless shelters located in urban areas, there can be an opportunity for intervention to help those dealing with a primary disease state to possibly receive adequate treatment and prevent hospitalizations.
Specific Risks in Homeless Populations
The death toll of cardiovascular disease in homeless populations drastically exceeds that of non homeless and that may be due to some unique barriers in the homeless population. The biggest barrier to care is transportation. 6 Most people utilize the bus system but on the days that they miss the bus or the services aren’t available on a particular day, it becomes increasingly hard to get where they need to go let alone see a physician. Without a reliable transportation method, most patients living in homelessness may not be able to follow up with a physician or pharmacist on a regular basis, leading to further mismanagement of important disease states. People living in homelessness also suffer from malnutrition where some may only have access to one meal a day. 6 This puts them at a particular risk of hypoglycemia, a fatal condition resulting from accelerated heart rate and low blood sugar, in addition to the other cardiovascular risk factors. Some medications and therapies require a specific diet regimen such as Type 2 Diabetes Mellitus, and without a proper source of nutrition the therapies a physician or pharmacist recommend could be rendered useless. There is also the lack of health insurance or stable income to pay for proper medical services. 6 While many may be supported by Medicaid, there could be a limited selection of medications that can be covered which can impact an ideal therapy. Furthermore, the prevalence of cigarette smoking in this population is upwards of about 80% which is a huge modifiable risk factor and opportunity for intervention to prevent further complications. 7 The absence of communication with these individuals, cost, transportation, diet, and many more provide unique barriers that health care professionals will constantly need to navigate through to provide ideal care.
7 Centers for Disease Control and Prevention. Heart Disease Facts. https://www.cdc.gov/heartdisease/facts.htm. Accessed November 11, 2019.
Eskenazi Health
The mission of Eskenazi Health is to advocate, care, teach, and serve with special emphasis on the vulnerable populations. 8 They have been heavily involved with serving people who do not have access to health care and continuously work with them to make sure that there are no barriers to taking care of their health. They work with issues of location, and finances to help under served individuals take charge of their heath. Eskenazi Health has continued to make innovative strides in patient care and one example of this implementation with their ambulatory care pharmacies. 8
Cardiovascular Risk Reduction Ambulatory Care Pharmacy
Ambulatory care pharmacists have been the front lines in helping patients manage their primary disease states including but not limited to dyslipidemia, hypertension, type II diabetes, smoking cessation and asthma. They work in a physician’s office and meet one on one with patients to help educate them on medications, and lifestyle habits to help promote healthy lifestyles. Appointments typically last about an hour and they are very personal interactions that have seen great benefit in outcomes such as reduction in A1c, blood pressure, lipid levels, and an increase in the desire to quit smoking. Pharmacists interventions can be essential in helping to reduce cardiovascular events, and Eskenazi has done an outstanding job of implementing these into various clinics.
The Pedigo Clinic
The ambulatory care clinics with Eskenazi Health have been a front runner in cardiovascular risk reduction strategies through interventions from a team of healthcare professionals ranging from dietitians to pharmacists. An ambulatory care pharmacist can be on the front lines of care for a patient with the ability to sit down and have an hour one on one discussion about disease risk factors, how to modify them with both lifestyle and pharmacological changes, and planning for their long term health goals. Eskenazi Health has seen significant improvements in patient’s health with ambulatory care pharmacists and now the Pedigo Clinic, a clinic that focuses predominantly on homeless populations, is seeking to implement a cardiovascular risk reduction service to those patients who need it. Considering the following cardiovascular statistics in Indiana, it is imperative to reduce the risk of cardiovascular events, especially in the homeless populations.
References:
1 Centers for Disease Control and Prevention. Heart Disease Facts. https://www.cdc.gov/heartdisease/facts.htm. Accessed November 11, 2019.
2 What is Cardiovascular Disease? American Heart Association website. https://www.heart.org/en/health-topics/consumer-healthcare/what-is-cardiovascular-disease. Accessed November 13, 2019.
3 Indiana State Fact Sheet. American Heart Association website. https://www.heart.org/-/media/files/about-us/policy-research/fact-sheets/quality-systems-of-care/quality-systems-of-care-indiana.pdf?la=en&hash=96D09D01F6D4695F675C6807B795D1B678A3814A. Accessed November 15, 2019
4 American College of Cardiology. Homeless Populations at High Risk to Develop Cardiovascular Disease. https://www.acc.org/about-acc/press-releases/2018/05/29/10/08/homeless-populations-at-high-risk-to-develop-cardiovascular-disease. Accessed November 12, 2019.
5 United States Interagency Council on Homelessness. Indiana Homeless Statistics. https://www.usich.gov/homelessness-statistics/in/. Accessed November 8, 2019.
6 Jones CA, Perera A, Chow M, Ho I, Nguyen J, Davachi S. Cardiovascular disease risk among the poor and homeless – what we know so far. Curr Cardiol Rev. 2009;5(1):69–77. doi:10.2174/157340309787048086
7 Baggett TP, Liauw SS, Hwang SW. Cardiovascular Disease and Homelessness JACC. 2018;17(22):2585-2597. doi.org/10.1016/j.jacc.2018.02.077
8 About page. Eskenazi Health website. https://www.eskenazihealth.edu/about Accessed November 8, 2019.