
Location:
- Located within the Eskenazi Health – Pedigo Health Center
- Connected to Horizon House – a facility that provides aid to the homeless population with resources, relationships, and life skills
- Clinic Hours
- Tuesday & Friday: 8:00 am – 5:00 pm
- Clinic is already established with exam rooms, medication rooms, work space, and computers.
Staffing Requirements:
- Half of an FTE — ambulatory care pharmacist working 8 am – 5 pm
- Requirements include 1) PharmD, 2) PGY1, and 3) PGY2 in Ambulatory Care/Primary Care/Pharmacotherapy -or- currently completing an Eskenazi Health PGY2 Ambulatory Care Pharmacy Residency.
- Clerical staff already in place with existing clinic
- Will aid in scheduling patients and reminder calls
Referral Process:
- Self-referred, or referred through the Horizon House
Barriers specific to Pedigo Clinic:
- Storage
- Pharmacist will have to understand that storage for medications is difficult with this population and determine a way to keep refrigerated medications, like insulin, efficacious, especially during the winter months.
- Pharmacist will have to work on the medication room to make the process more efficient and less prone to regulatory issues.
- Adherence
- Pharmacist will have to educate patient on importance of adherence and try to decrease barriers that lead to decreased adherence, such as:
- Physical cost to travel to the off-site pharmacy
- Pharmacist will have to organize medication regimens to 1 or 2 weeks of days supply.
- Pharmacist will have to educate patient on importance of adherence and try to decrease barriers that lead to decreased adherence, such as:
- Health Literacy
- Pharmacist will have to understand what resources are available to this specific population and what resources are most important for this population.
- Administration
- Pharmacist will have to educate patient on administration of medications in clinic, such as insulin.
- Housing, Meals, Etc.
- Pharmacist will have to work with Horizon House staff and the social worker on site to help patient find the resources they need.
- Vaccinations
- Pharmacist will have to make sure patients are up to date with their vaccinations with their disease states.
- Pharmacist will have to recommend vaccinations to patients, if needed be and then administer them.
- Hepatitis C Management
Billing Processes:
- Fixed rate for reimbursement for patients with Medicaid regardless of level of service provided
- Level 3 or 4 for Medicaid = $304
- Medicaid – primary insurance used at clinic (FQHC)
- Level 5 with shared
- Level 3/4 with only physician
- No billing for independent visits
Patient Visits:
- Shared visits vs. independent pharmacist visits:
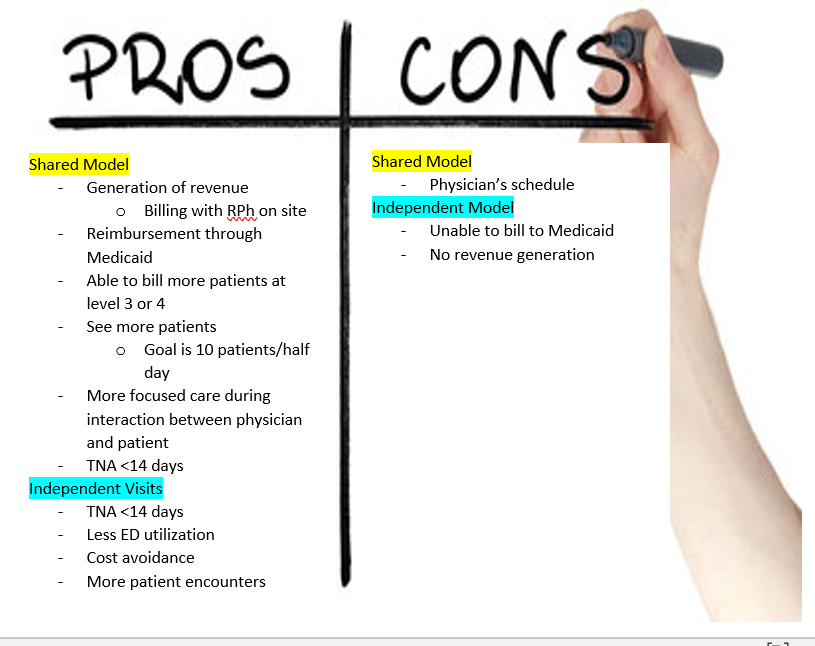
- 1/2 a day with shared visits
- 10 patients with physicians vs. 5 patients on own
- 1.5 days with independent model
- 15 patients altogether
Pharmacist – Patient Interaction:
- CVRR management
- Management of diabetes, hypertension, dyslipidemia, and tobacco cessation per CDTM.
- Asthma and COPD management
- Initial and follow up visits may include any of the following:
- Patient will meet with the pharmacist within the clinic.
- Pharmacist will explain the purpose of the visit.
- Pharmacist will do a medication reconciliation with each of the medications patient is on.
- Any changes in adverse effects, any concerns from the patient regarding their disease states, missed doses, storage issues, etc.
- Pharmacist reviews patient’s disease states and medications prescribed looking to optimize therapy by reducing duplicate therapy and preventing adverse effects.
- Pharmacist will alter medication regimen using lab values and goals based on guidelines that are established in the CDTM.
- Pharmacist will educate on disease state, current medication side effects, storage, and additional monitoring.
- Pharmacist will educate on lifestyle modifications and considerations.
- Pharmacist to schedule follow-up appointment at the end of the initial visit.
- Initial and follow up visits may include any of the following:
Scope of practice and Pharmacologic Privileges:
- Independent – no routine provider consultation required
- Antidiabetic agents – oral and injectable
- Antihypertensives and diuretics
- Antilipidemic agents
- Diabetic and blood pressure supplies
- Insulins (with the exception of Humulin R U-500 Insulin)
- Nicotine replacement products and medications to aid in smoking cessation
- OTC medications
- Vaccines
- Inhaled beta-2 agonists and combination products
- Inhaled corticosteroids and combination products
- Inhaled anticholinergics and combination products
- Inhaler/nebulizer supplies
- Phosphodiesterase-4 Inhibitors
- Provider consultation required for initiating therapy – independent for renewing and adjusting
- Antidepressants for neuropathy
- Anticonvulsants for neuropathy
- Humulin R U-500 Insulin
- Oral corticosteroids
- Independent (pursuant to treatment guidelines) for renewal only
- Antiplatelets
Visit Documentation:
- Documentation of all visits will be done on Eskenazi’s electronic medical record (EPIC).
- Recommendations for adjustment in therapy
- Interventions for patient’s compliance
- All providers will be able to stay informed on patient progression through EMR.
- Notes on all patients seen that day will be updated and available for all providers to review at the end of each clinic day.
Data Measures:
- Pilot Pedigo Clinic’s success will be measured utilizing retrospective data looking at cost avoidance specifically regarding:
- Time to Next Available Appointment (TNA)
- ED readmission rates
- Clinical values
- Smoking status
- BP <130/80 mmHg
- BMI
- A1C < 8
- Lipid levels
- Documented in EMR for each visit
- Change in clinical values related to specific disease state being managed
- Patient reported ED visits and hospitalizations related to one of the five disease states listed under CDTM
- Patient’s vaccination history
- Pharmacist’s progress note, including all the recommendations made
Interventions:
- Medication Reconciliation
- Recommend and adjust medications based on current guidelines in the CDTM and physician recommendations
- Vaccination recommendations and reconciliations
- Drug Interaction screenings
- Education regarding HTN, DM, smoking, and dyslipidemia
- Assistance in medication dosing, selection, titration, and ordering.
- Assistance with PAs/facilitation with nursing PA coordinator or MDs unsure of rejections
- Contact pharmacy to ensure delivery of medications to improve adherence.
Patient Discharge from CVRRC
May include, but are not limited to the following:
- Achievement of all relevant clinical goals
- Consistent failure to keep appointments
- Threatening or abusive behavior
- The patient decides to opt-out of CVRRC services
- The patient’s provider opts-out of having his/her patient enrolled in CVRRC services
The pharmacist documents reason for discharge in the patient’s electronic medical record and notifies patient, as appropriate.
Established Collaborative Drug Therapy Management Protocol (CDTM):
- The following guidelines should be used in the management of patient’s disease states:
| Diabetes Mellitus | American Diabetes Association (ADA) |
| Hypertension | ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA
Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults |
| Hyperlipidemia | AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCN A guideline on the Management of Blood Cholesterol
AAC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease |
| Tobacco Cessation | US Department of Health and Human Services, Treating Tobacco Use and Dependence |
| Asthma | National Asthma Education and Prevention Program (NAEPP) |
| COPD | Global Initiative for Chronic Obstructive Lung Disease (GOLD) |