

Incidence and Prevalence:
Hepatitis C is a prevalent health condition in today’s world. In 2014, a total of 2,194 cases of acute hepatitis C were reported to the CDC, with an overall increased incidence rate from 2010-2012 with 0.7 cases per 100,000 population. Currently, 2.7-3.9 million people in United States have chronic hepatitis C.1
In 2015, the number of acute hepatitis C cases in Indiana increased by 13.1% from 122 cases in 2014 to 138 cases. This was due largely to injection drug use, the primary risk factor for an outbreak of HIV in Scott County.2
 Prevalence of both acute (confirmed) and chronic (confirmed and probable) hepatitis C cases in Indiana reported during 2015 (including IDOC sites). Some of the rates are based on fewer than 20 counts and should be considered unstable.2
Prevalence of both acute (confirmed) and chronic (confirmed and probable) hepatitis C cases in Indiana reported during 2015 (including IDOC sites). Some of the rates are based on fewer than 20 counts and should be considered unstable.2
How Does Hep C Work?
https://www.youtube.com/watch?v=VNe0SJnWckQ
Who is at Risk? Who are we Treating?
- Injection Drug Users
- Approximately 1/3 of IDUs aged 18-30 have HCV
- 70-90% of older and former IDUs have HCV
- Recipients of blood transfusions or solid organ transplant before 1992
- Recipients of clotting factor concentrates made before 1987
- Chronic hemodialysis patients
- Persons with known exposures to HCV
- Health care workers with needle stick involving HCV (+) blood
- Recipients of HCV (+) blood or organ donation
- HIV patients
- Children born to HCV (+) mothers1
Chronic Disease Management
15-25% of persons infected can clear the virus without treatment; however, 75-85% of cases become chronic. Many chronic cases are asymptomatic, and symptoms may not appear for up to 24 weeks post-exposure. Hepatitis C infection is the leading cause for liver transplantation in the US. If not treated, hepatitis C can lead to devastating long term consequences:1
Of every 100 persons infected with HCV:
- 60-70 will develop chronic liver disease
- 5-20 will develop cirrhosis over a period of 20-30 years
- 1-5 will die from consequences of chronic infection (liver cancer or cirrhosis)
19,659 deaths associated with HCV were reported in 2014.1 While there is no vaccine for hepatitis C, patients can be cured utilizing the new and highly specialized drugs available. With the proper guidance by a patient’s health care team, including medication counseling by a clinical pharmacist, a cure and a happier, healthier life is entirely possible.
Why A Clinic?
Evidence to Support a Pharmacist-Run Hepatitis C Ambulatory Care Clinic:
Preventive Care
- Increasing public and individual awareness about HCV prevalence and transmission
- Vaccinations
- Vaccination against hepatitis A and B recommended for all susceptible persons with HCV infection4
- Vaccination against pneumococcal infection recommended to all patients with cirrhosis4
Improved Medication Adherence
- Pharmacists are more accessible providers with more time available to dedicate to patient interaction
- Patients would be able to contact the pharmacist easily should anything arise that could interfere with their ability to complete the drug regimen5
- Use of a clinical pharmacist has shown to encourage therapy adherence and have a positive impact on SVR in Hepatitis C patients5,6
Improved Patient Satisfaction
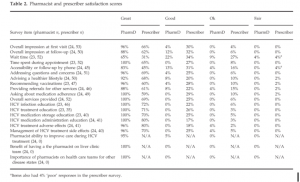
- Compared to prescribers, pharmacists had higher patient satisfaction scores in areas including overall impression at initial and subsequent visits, time spent during appointment, accessibility or follow-up by phone and education on disease state and medications. Other improved patient satisfaction areas are listed in the tables below.
- Pharmacist and prescriber satisfaction scores:5
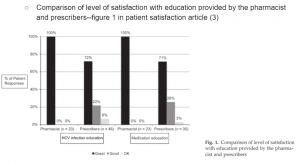
- Comparison of level of satisfaction with education provided by the pharmacist and prescribers:5
Increase Amount of Patients Initiated on Therapy Without Overburdening Existing Medical HCV Providers
- Pharmacists at an adult ambulatory care HCV clinic within the Miami Veterans Affairs Health Care System initiated over 500 patients on HCV treatment with SVR-12 rates over 90%4
- Patients can be assessed and monitored by diagnostic and pharmacotherapy experts when pharmacists are utilized4
- Pharmacists are able to remove the strain of HCV follow-up appointments from prescribers’ schedules and help develop supportive patient-provider relationships5
Assist in Monitoring Clinical and Adverse Effects
- Genotyping of HCV
- Monitoring viral load
- NS5A resistance testing or testing avoidance where appropriate
- Identifying medication side effects and side effect management
Reduce Patient and Health Care System Costs
- New antiviral agents are becoming increasingly available but are extremely costly for patients and the health care system
- Utilizing an interprofessional approach including a pharmacist has achieved more quality-adjusted life-years and lower costs than a control group of hepatologists in the management of HCV6
Constantly Evolving Medication Regimens
- Pharmacists are uniquely qualified to stay up-to-date on new medications for the management of hepatitis C while also analyzing patients’ concomitant disease states, interactions, and adverse effects
- The demand for HCV treatment is predicted to increase as newer medications are associated with higher SVR rates and less side effects. With an increasing patient load, pharmacists can help reduce the burden on other HCV providers while optimizing patient therapy7
Summary Info Graphic Courtesy of the VA:
hepatitisC-infographic from VA (8)
-
Viral hepatitis-Hepatitis C information. Centers for disease control and prevention (CDC) website. https://www.cdc.gov/hepatitis/hcv/hcvfaq.htm. January 27, 2017. Accessed February 11, 2017.
-
Indiana State Department of Health. Annual report of infectious diseases 2015. http://www.in.gov/isdh/files/2015%20ISDH%20Annual%20Report%20of%20Infectious%20Diseases.pdf. December 2016. Accessed: February 10, 2017.
-
American Association for the Study of Liver Diseases (AASLD) and Infectious Diseases Society of America (IDSA) Recommendations for Testing, Managing, and Treating Hepatitis C : http://www.hcvguidelines.org/full-report/initial-treatment-hcv-infection.
-
Gauthier TP, Moriera E, Chan C, et. al. Pharmacist engagement within a hepatitis C ambulatory care clinic in the era of a treatment evolution. JAphA. 2016;56(6):670-676. doi:10.1016/j.japh.2016.06.013.
-
Martin MR, Faber DM. Patient satisfaction with the clinical pharmacist and prescribers during hepatitis C virus management. J Clin Pharm Ther. 2016;41(6):645-649. doi:10.1111/jcpt.12436.
-
Wenzler E, Dickson W, Vighakar S, Adeyemi OM, Danziger LH. Hepatitis C management and the infectious disease pharmacist. Clin Infect Dis. 2016;61(7):1201-1202. doi:10.1093/cid/civ545.
-
Mohammad RA, Bulloch MN, Chan J, et. al. Provision of clinic pharmacist services for individuals with chronic hepatitis C viral infection. Pharmacotherapy. 2014; 34(12):1341-1354. doi:10.1002/phar.1512.
-
Don’t let hepatitis c surprise you. US Department of Veterans Affairs website. http://www.hepatitis.va.gov. June 2015. Accessed: February 11, 2017.